The Neurodivergent Survival Cycle: A Neuroaffirming Framework for Understanding Chronic Stress, Shame, and Burnout
 The Neurodivergent Survival Cycle: A Neuroaffirming Framework for Understanding Chronic Stress, Shame, and Burnout
The Neurodivergent Survival Cycle: A Neuroaffirming Framework for Understanding Chronic Stress, Shame, and Burnout
Mental health professionals are increasingly working with Autistic, ADHD, and AuDHD clients who arrive in therapy carrying profound exhaustion, shame, confusion, and chronic overwhelm. Many have spent years trying to adapt to environments that were never designed with their neurotype in mind. Yet these experiences are still too often conceptualized through an individual-deficit lens rather than within the broader context of systemic ableism, chronic invalidation, and survival adaptation.
The Neurodivergent Survival Cycle offers clinicians a neuroaffirming framework for understanding how repeated exposure to stigma, rejection, sensory overwhelm, and pressure to conform can shape a neurodivergent person’s nervous system, identity, coping strategies, and wellbeing over time.
Rather than viewing distress solely as pathology located within the individual, this model highlights how chronic environmental mismatch and discrimination contribute to many of the mental health challenges neurodivergent people experience. It also helps explain why so many clients present in therapy with burnout, trauma symptoms, self-criticism, emotional dysregulation, masking fatigue, and disconnection from their needs and identity.
Understanding the Neurodivergent Survival Cycle
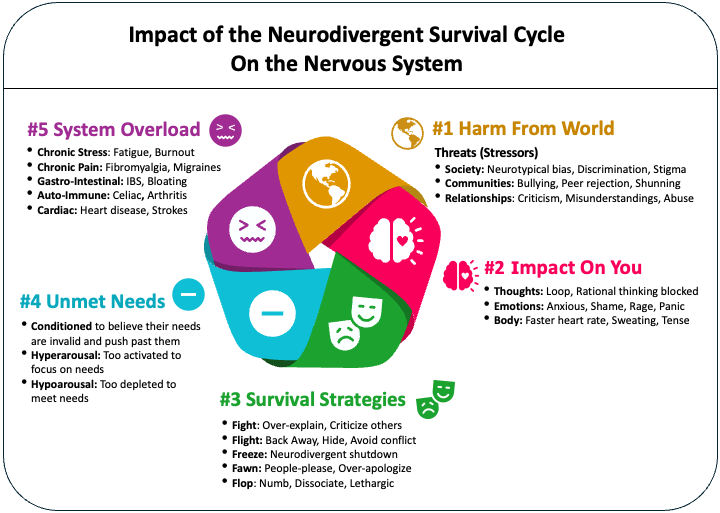
The Neurodivergent Survival Cycle conceptualizes neurodivergent distress as a series of interconnected layers that continuously influence one another rather than a simple linear progression.
The five layers include:
- Harm from the world
- Impact on the self
- Survival responses
- Unmet needs
- System overload
Together, these layers illustrate how chronic exposure to ableism and invalidation can gradually erode self-trust, increase survival-based coping, and push the nervous system toward exhaustion and burnout.
For therapists, this framework can support more compassionate case conceptualization, reduce pathologizing interpretations, and help clients externalize shame.
Layer 1: Harm from the World
The first layer acknowledges a reality often minimized in traditional mental health frameworks: Autistic and ADHD individuals frequently encounter chronic adversity while navigating neurotypical systems and expectations.
Research consistently demonstrates elevated rates of:
- Peer victimization
- Social exclusion
- Sensory trauma
- Caregiver misunderstanding or abuse
- Bullying
- Discrimination
- Chronic invalidation
These experiences often begin early in childhood and continue across school, healthcare, workplace, and relational environments.
The Role of Ableism
Ableism refers to prejudice, discrimination, and systemic barriers directed toward disabled and neurodivergent people. Within neurodivergent populations, ableism may show up through:
- Pressure to appear “normal”
- Punishment for sensory or communication differences
- Pathologizing natural neurodivergent traits
- Viewing accommodations as inconveniences
- Assuming incompetence or laziness
- Prioritizing neuronormative behavior over wellbeing
Many neurodivergent clients internalize these messages over time. They may come to believe they are “too much,” “not enough,” broken, incompetent, dramatic, lazy, selfish, or fundamentally defective.
This internalization process is clinically significant. Therapists may encounter clients who present with intense self-blame while having limited awareness of the systemic harms contributing to their distress.
Systems as Chronic Stressors
School systems, healthcare systems, workplaces, and social institutions often reward neurotypical communication, sensory tolerance, productivity patterns, and relational norms.
Examples include:
- Expectations for sustained eye contact
- Punishment for movement or stimming
- Overreliance on verbal processing
- Sensory-overloading environments
- Complex bureaucratic processes requiring executive functioning
- Social demands that privilege masking over authenticity
Many neurodivergent individuals spend years adapting themselves to systems instead of systems adapting to them.
From a trauma-informed perspective, these experiences are often repetitive, chronic, and cumulative rather than isolated incidents.
The Double Empathy Problem
One particularly important concept for therapists is the Double Empathy Problem, introduced by Damian Milton (2012).
Traditional deficit-based models often assume Autistic people struggle with empathy or perspective-taking. The Double Empathy framework challenges this assumption by proposing that misunderstandings arise mutually between people with different neurotypes.
In other words, communication breakdowns are not simply caused by Autistic deficits. Rather, both individuals may struggle to intuitively understand one another because they operate from different assumptions, communication styles, sensory experiences, and relational expectations.
This framework can profoundly shift therapeutic work.
Many neurodivergent clients enter therapy believing they are solely responsible for interpersonal difficulties. They may automatically assume:
- “I’m the problem.”
- “I misunderstood.”
- “I hurt them.”
- “I’m difficult.”
- “I’m stupid.”
Repeated exposure to blame and misunderstanding can reinforce shame-based identity structures and hypervigilance within relationships. Therapists who understand the Double Empathy Problem are often better positioned to help clients move away from chronic self-pathologizing.
Minority Stress and Neurodivergence
The Neurodivergent Survival Cycle aligns closely with the Minority Stress Model, which explains how marginalized groups experience chronic stress related to stigma, discrimination, concealment, rejection, and internalized oppression.
Although originally developed in research on racial and sexual minorities, this framework has increasingly been applied to Autistic and ADHD populations.
Research suggests neurodivergent individuals frequently experience:
- Anticipation of rejection
- Concealment of identity
- Internalized stigma
- Discrimination and victimization
- Chronic social vigilance
Importantly, these stressors predict poorer mental health outcomes, including anxiety, depression, posttraumatic stress, and burnout.
For therapists, this means many neurodivergent clients are not coping with the cumulative effects of living within environments that repeatedly communicate that their authentic way of being is unacceptable.
Layer 2: Impact on the Self
The second layer focuses on how chronic harm from the environment shapes a neurodivergent person’s internal world.
Repeated experiences of criticism, invalidation, rejection, exclusion, or coercion can significantly affect:
- Self-worth
- Identity development
- Emotional regulation
- Nervous system functioning
- Core beliefs
- Sense of safety
Shame and Internalized Ableism
Many neurodivergent clients carry deep shame related to:
- Productivity
- Social performance
- Emotional intensity
- Support needs
- Sensory sensitivities
- Executive functioning struggles
- Communication differences
Over time, external messages may transform into internal narratives:
- “I’m defective.”
- “I’m a burden.”
- “I’m too sensitive.”
- “I’m failing at life.”
- “I’m fundamentally wrong.”
These beliefs often coexist with chronic rumination, shame spirals, self-criticism, and anticipatory anxiety around future rejection.
Emotional and Physiological Impact
Therapists may also notice that neurodivergent clients frequently describe intense or complex emotional states accompanied by strong physiological activation.
Experiences of rejection or invalidation may trigger:
- Chest tightness
- Dissociation
- Shaking
- Nausea
- Emotional flooding
- Shutdown
- Cognitive fog
- Numbing
- Panic responses
For some clients, these responses are compounded by rejection sensitivity, trauma histories, sensory overload, or chronic nervous system dysregulation.
Clinicians who interpret these reactions solely as emotional dysregulation due to neurodivergence may miss the broader context: many neurodivergent nervous systems have adapted to years of threat, unpredictability, and invalidation.
Layer 3: Survival Responses
The third layer explores the adaptive strategies neurodivergent people develop in response to chronic stress and social danger.
These strategies are often misunderstood clinically. What may appear “maladaptive” is frequently protective.
Masking and Camouflaging
Masking refers to suppressing or hiding neurodivergent traits to appear more neurotypical. Camouflaging includes broader strategies used to blend in socially, compensate for differences, or avoid exclusion.
Examples may include:
- Forcing eye contact
- Suppressing stims
- Rehearsing conversations
- Mimicking others’ body language
- Over-monitoring social behavior
- Hiding interests or needs
- Performing socially acceptable personas
Clients often describe masking as exhausting but necessary for survival.
Importantly, research suggests camouflaging is associated with increased anxiety, stress, depression, trauma symptoms, and burnout.
Other Common Survival Strategies
Therapists may also observe:
- People-pleasing or fawning
- Perfectionism
- Overworking
- Hyper-independence
- Chronic over-explaining
- Avoidance
- Dissociation
- Emotional shutdown
- Over-preparation
- Silence around needs
These strategies often emerge because authenticity previously resulted in punishment, shame, exclusion, or danger.
Rather than asking clients to immediately stop these behaviors, neuroaffirming therapy recognizes that these adaptations likely developed for good reasons.
Layer 4: Unmet Needs
One of the most clinically important aspects of the Neurodivergent Survival Cycle is the chronic suppression or invalidation of neurodivergent needs.
Many Autistic and ADHD individuals grow up learning that their needs are:
- Inconvenient
- Excessive
- Dramatic
- Irrational
- Embarrassing
- Burdensome
As a result, clients may become profoundly disconnected from their internal signals and support needs.
Access Needs Are Real Needs
Neurodivergent access needs are not preferences. They are legitimate supports required for wellbeing and functioning.
These may include:
- Reduced sensory input
- Recovery time after social interaction
- Written communication
- Predictability and routine
- Movement and stimming
- Flexible scheduling
- Extra processing time
- Solitude
- Direct communication
- Environmental accommodations
When these needs are repeatedly ignored or dismissed, clients may stop recognizing their own limits until their nervous system reaches overload.
Supporting clients in understanding their sensory profile and neurodivergent needs is essential to supporting nervous system and emotional regulation, preventing and recovering from burnout, and building a positive neurodivergent identity.
Layer 5: System Overload
The final layer reflects the cumulative effects of chronic stress, masking, unmet needs, trauma, and nervous system dysregulation.
Eventually, many neurodivergent individuals reach a point where the body can no longer sustain the load.
This may present clinically as:
- Burnout
- Chronic fatigue
- Anxiety
- Depression
- Trauma symptoms
- Dissociation
- Sleep disturbances
- Gastrointestinal issues
- Chronic pain
- Emotional shutdown
- Executive functioning collapse
- Suicidality or hopelessness
Research suggests Autistic and ADHD individuals are at elevated risk for PTSD, chronic stress-related health conditions, and burnout.
From a neuroaffirming perspective, burnout is often the predictable outcome of prolonged survival in invalidating environments.
Clinical Implications for Therapists
The Neurodivergent Survival Cycle encourages therapists to move away from deficit-based interpretations and toward contextualized, systemic, and compassionate understandings of distress.
This framework may help clinicians:
- Reduce client shame and self-blame
- Better understand masking and burnout
- Normalize survival adaptations
- Recognize the impact of ableism and minority stress
- Support clients in reconnecting with needs and identity
- Shift treatment goals toward sustainability and authenticity
Perhaps most importantly, it reminds clinicians to see how many of the depressive, anxiety, burnout, OCD and other symptoms neurodivergent client are experiencing are driven by systemic and environmental factors.
Moving Beyond Survival
Healing for many neurodivergent clients often involves rebuilding self-trust, reclaiming identity, reconnecting with the body, and learning that their needs are valid.
Research increasingly suggests that positive neurodivergent identity and community connection are associated with improved wellbeing, self-esteem, and reduced anxiety and depression.
Therapy can become a powerful corrective experience when clinicians:
- Validate neurodivergent experiences
- Understand systemic contributors to distress
- Support nervous system regulation
- Honor access needs
- Reduce pathologizing interpretations
- Foster self-compassion and identity development
The Neurodivergent Survival Cycle offers therapists a framework for seeing neurodivergent distress not as evidence of pathology, but as evidence of adaptation, endurance, and survival within systems that too often fail to provide safety, accommodation, and belonging.
Authors –
Tasha Oswald, PhD and Cindy Brown, LPCC

